Recent changes in the guidelines of EAU (European Association of Urology) and the ACR (American College of Radiology) state the integration of prostate MRI in the diagnostic workflow as a standard in the Prostate Cancer (PCa) diagnostic workflow. The integration of prostate MRI into the diagnostic process could safely lead to avoidance of (unnecessary) biopsies, reduction of irrelevant cancer detection, and to accurate guidance in those cases where further biopsy is needed1.
Nowadays, prostate MRI plays a dominant role in early detection of PCa. Early detection gets more and more attention as it has been shown that risk assessment with MRI can positively change the equation of harms and benefits in PCa diagnosis2.
However, as every abdomen radiologist can attest, the assessment of multiparametric MRIs (mp-MRI) can be very challenging due to different factors. Reading mp-MRI can be difficult for all the different sequences that need to be taken into account and because of the level of experience required to see abnormalities with the naked eye. Additionally, radiologists require anatomical measurements of the prostate which may require the support from extra software.
As part of this process, determining the PI-RADS score of the suspected lesions can be one of the most challenging tasks for radiologists. It requires vast experience as the assessment can be relative to the skill of the radiologist’s on call3. Fortunately, artificial intelligence (AI) can be a useful asset in supporting one or multiple steps of the process.
Discover how AI can support PI-RADS scoring
For those reasons, we have prepared the following article explaining what a PI-RADS score is, its importance and how AI can support PI-RADS scoring to make the process of reading MRI easier and more efficient for the radiologist.
PI-RADS scoring
Prostate Imaging Reporting and Data System (PI-RADS) is a classification system for prostate MRI that was first introduced in 2012 in search of a “more standardized acquisition, interpretation and reporting of prostate MRI. Subsequently, this classification system has developed over the years into the most recent version”4. Depending on its likelihood of being significant PCa, radiologists will assign a score (from 1 to 5) to a lesion using the information and analyses of different of mp-MRI sequences.
As with every step of the diagnostic process, a solid PI-RADS assessment is essential to aid urologists in making correct diagnostic and treatment decisions. As an example, while the standard threshold still remains undecided, lesions with a PI-RADS score higher than 3 are generally indicated to biopsy. Hence, differentiating between lower PI-RADS scores and higher PI-RADS scores has direct influence on the course of the diagnostic process and therefore indirectly on the diagnosis itself5.
What does a PI-RADS score exactly mean?
PI-RADS scores in itself are easy to understand. There are five different scores that can be assigned to a lesion:
- PI-RADS score 1: Very low (clinically significant cancer highly unlikely)
- PI-RADS score 2: Low (clinically significant cancer unlikely)
- PI-RADS score 3: Intermediate (clinically significant cancer equivocal)
- PI-RADS score 4: High (clinically significant cancer likely)
- PI-RADS score 5: Very high (clinically significant cancer highly likely)
Step-by-step PI-RADS scoring on mp-MRI
Although PI-RADS is a structured system and a valuable step towards lowering the interobserver disagreements6, determining the right PI-RADS score is not an obvious task. The specific grade for a lesion depends on the T2w and the DWI scans and ADC scans, as well as the DCE sequence. Below we provide a step-by-step overview to get to a PI-RADS score. We will focus on the scoring of lesions in the transition and peripheral zone since this is where most lesions are located.
Step 1: Determine lesion zone
The main sequence needed for a correct assessment depends on the location of the lesion. For the transition zone (TZ) the T2w is the sequence primarily used for PI-RADS scoring, suspect lesions in the peripheral zone (PZ) require a thorough inspection of the DWI/ADC scans. Hence, it is essential to correctly determine the location of a lesion in order to accurately assign a PI-RADS score to it.
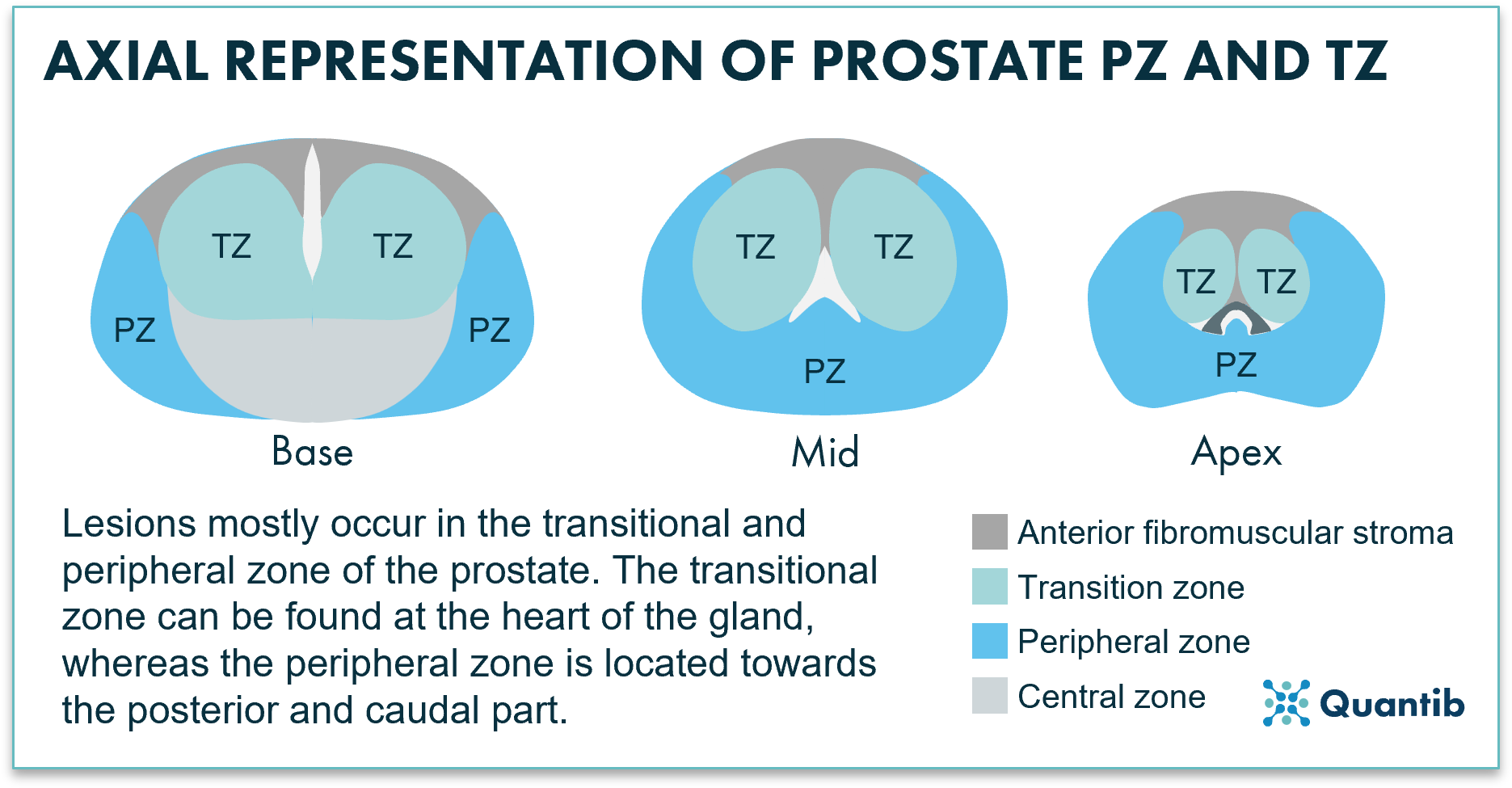 Figure 1: Axial representation of the prostate's peripheral and transitional zones.
Figure 1: Axial representation of the prostate's peripheral and transitional zones.
Step 2 in case of peripheral findings:
As mentioned, the DWI sequence and ADC map are leading for determining a PI-RADS score in the peripheral zone.
In case of a peripherally located lesion, what do you see on the ADC and DWI and what does this mean?
- Do you see a normal ADC and DWI? This means a PI-RADS score of 1.
- Is the suspect area on the ADC indistinct hypointense? This is a PI-RADS 2 lesion.
- Do you find a focal mild/moderate hypointense area on the ADC combined with an iso/mild hyper intense signal on the DWI, and is the lesion smaller than 1.5cm? Then check the DCE.
- Do you find no focal or early contrast-enhancement? This lesion should be assigned a PI-RADS score of 3.
- Do you find focal or early contrast-enhancement? This lesion should be assigned as a PI-RADS 4.
- A focal markedly hypointense ROI on the ADC and a markedly hyperintense region on the DWI, and a lesion smaller than 1.5cm? This should get a PI-RADS 4 score.
- Does it show everything as described for a PI-RADS 4 lesion but the largest dimension of the lesion is larger than 1.5cm? This is a PI-RADS 5 lesion. If there is extraprostatic extension (beyond the imaginary prostatic border or into the seminal vesicles), also the score 5 should be assigned.
Step 2 in case of transitional findings:
The transition zone mainly uses the T2w images to stage lesions, which are, as a final step, correlated with the information that can be obtained from the DWI and ADC.
What do you see on the T2w scan and what does this mean?
- A normal appearance in the T2 sequence means a PI-RADS score of 1.
- Are the regions of interest clearly circumscribed and hypointense or heterogeneous encapsulated? This indicates BPH nodules and a PI-RADS score of 2.
- Heterogenous signal intensity with obscured margins or lesions which do not fall in other categories require a check of the DWI sequence.
- Is the lesion in the DWI markedly intense but smaller than 1.5cm? This implies a PI-RADS 3 lesion.
- However, if the lesion appears markedly intense and the diameter is greater than 1.5 cm, the PI-RADS score will increase to 4.
- A lenticular or noncircumscribed, homogenous, moderately hypointense lesion which has a diameter smaller than 1.5cm indicates PI-RADS 4.
- Are all manifestations similar to what was described in the previous bullet as PI-RADS 4, but is the largest diameter of the area larger than 1.5 cm? This is a PI-RADS 5 lesion.
An overview of the PI-RADS scoring process can be found in figure 2.
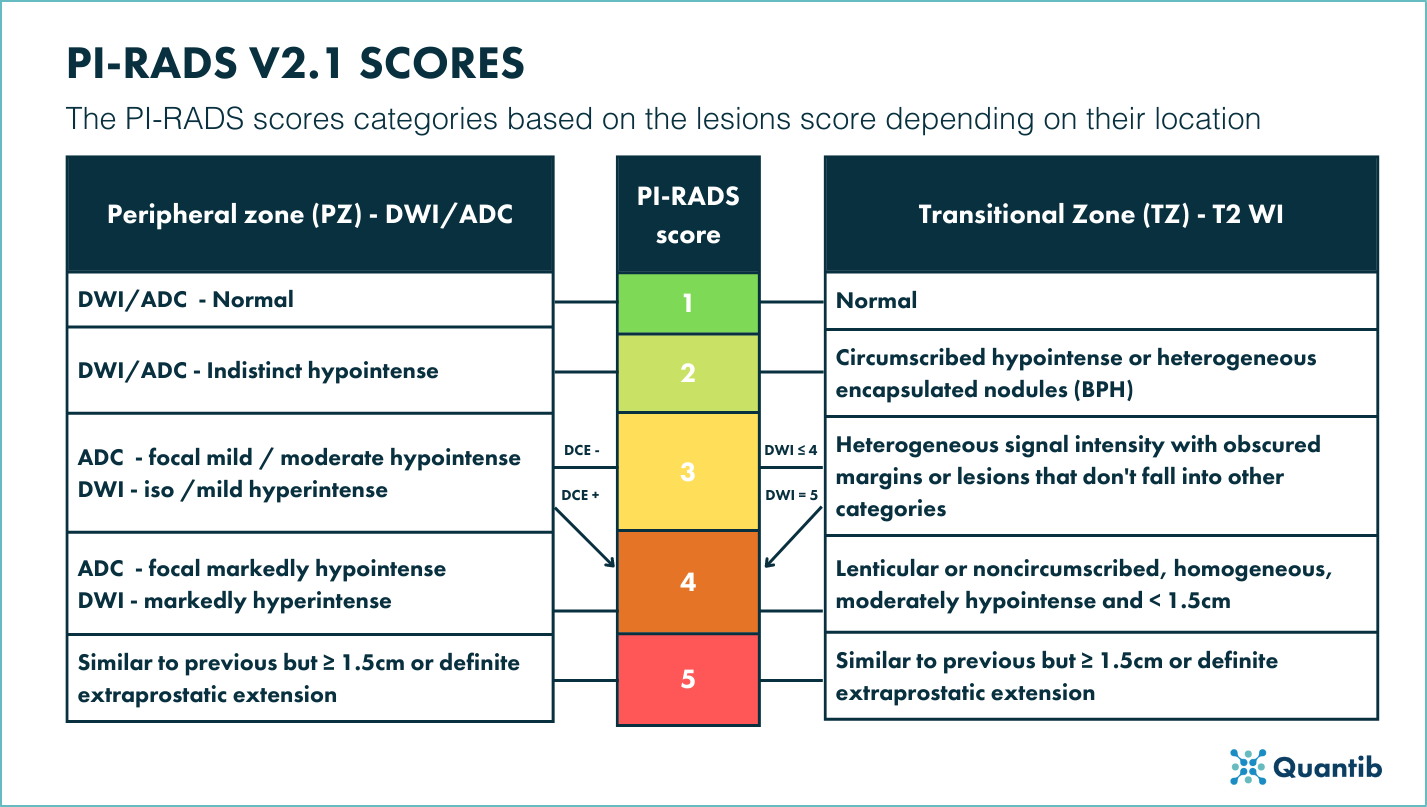 Figure 2:Table depicting PI-RADS v2.1 scores based on the findings on the transitional and peripheral zones.
Figure 2:Table depicting PI-RADS v2.1 scores based on the findings on the transitional and peripheral zones.
PI-RADS scoring on biparametric MRI (bp-MRI)
The PI-RADS v2.1 guidelines were constructed to aid the standardization of mp-MRI interpretation. However, these guidelines do not fit the interpretation of biparametric MRI. With the need of reaching a standardized system and methodology for the latter, several authors have pondered about it and proposed a simplified PI-RADS system or S-PI-RADS. As the name suggests, this classification scheme covers a simplified prostate imaging and reporting data system compared to PI-RADS v2.1.7.
Although the use of mp-MRI for prostate cancer diagnosis is not universally adopted and bp-MRI is often deployed as an alternative, it has to be said that the application of S-PI-RADS is controversial and not adopted by the PI-RADS steering committee. A schematic guideline of this system can be found in figure 2.
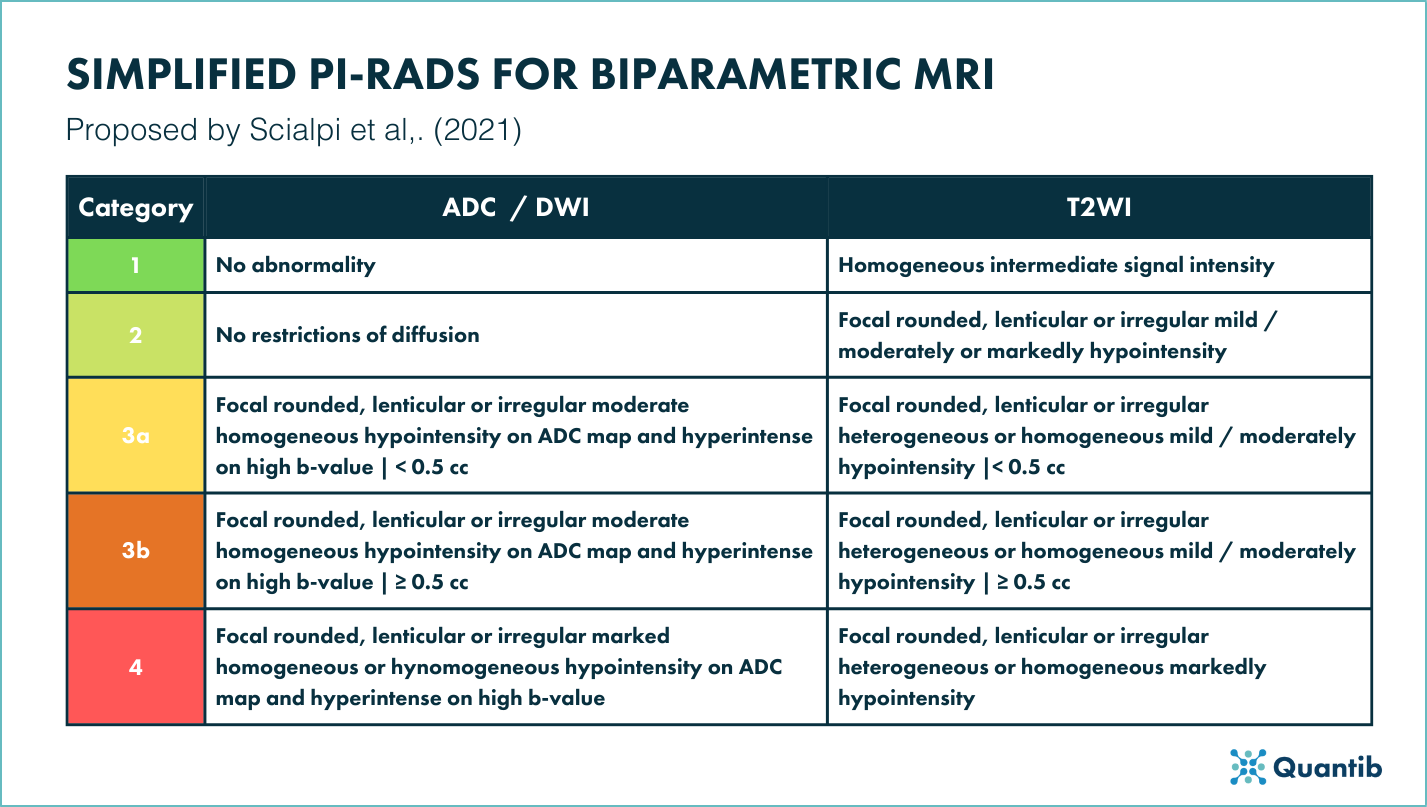 Figure 3: Table depicting the proposed simplified PI-RADS for bp-MRI adapted from7.
Figure 3: Table depicting the proposed simplified PI-RADS for bp-MRI adapted from7.
How does a PI-RADS score relate to a Gleason score?
The PI-RADS score is determined by a radiologist based on prostate MRI scans, whereas the Gleason score is set by the pathologist based on the results of prostate biopsies. While the radiology report provides a risk assessment of identifying clinically significant prostate cancer, the pathology exam confirms whether the biopsy samples contain cancerous tissue and provide a risk assessment for further treatment together with a prognosis. MRI assessments may have the ability to predict the outcome of the pathology evaluation, however, currently many researches are covering this topic and unfortunately it is to early for clinical practice to benefit from widely proven insights8.
How does the Gleason score work?
The pathologist will assign a score to the two most prevalent patterns of the prostate, or in cases where there is a more malignant pattern that is less prevalent, this will be graded as the secondary pattern, and they will be summed up to give the final Gleason score (i.e. 4 + 3 gives a Gleason score of 7 or if the sample mostly consists of pattern 3, then pattern 2 but there is also pattern 4, the resulting Gleason score will be 3 + 4 = 7). The higher the score, the more abnormal the pattern was found. Hence a higher Gleason score relates to a higher risk for the patient. See figure 3 for an overview of how to Gleason scores.
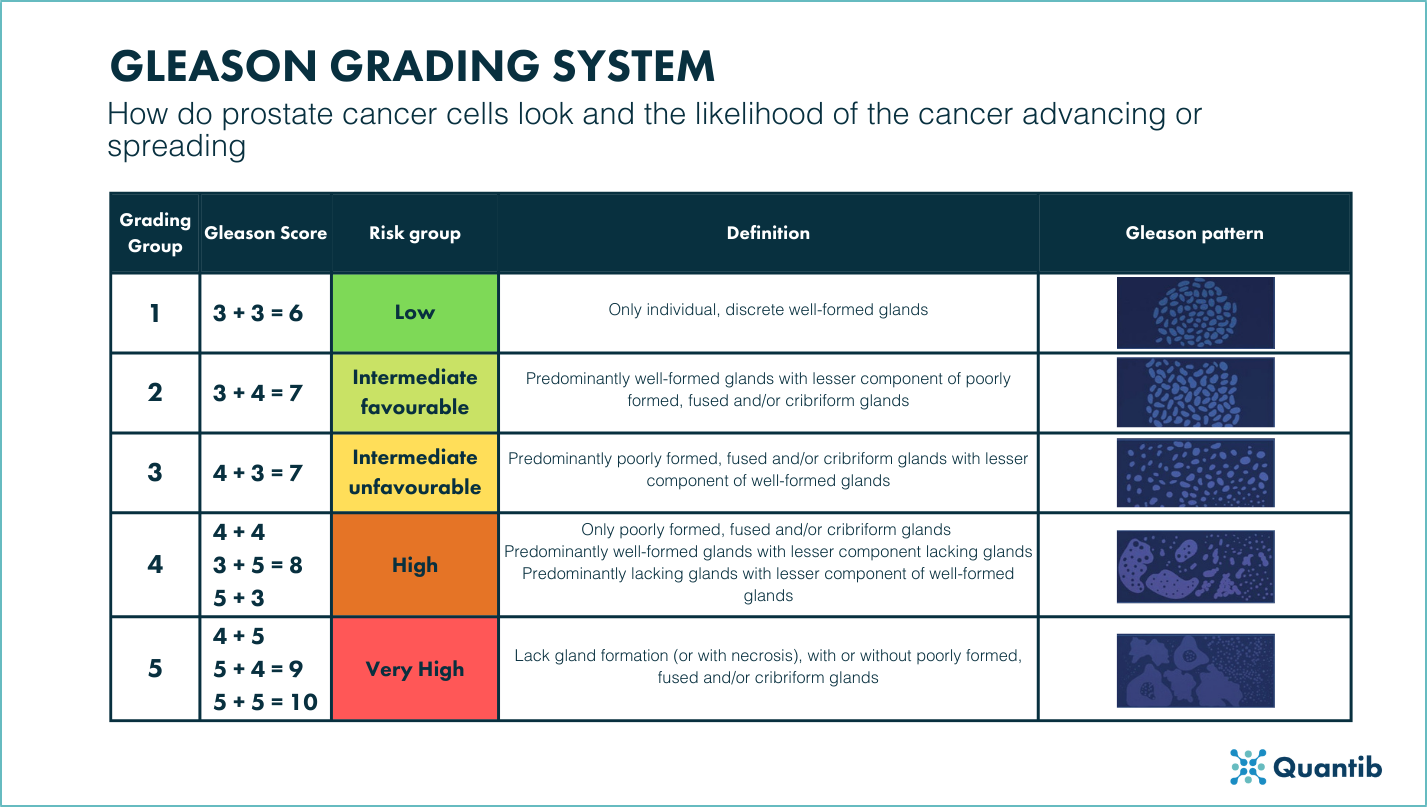
Figure 4: Table depicting the Gleason grade groups, the Gleason scores and the Gleason patterns currently used in the diagnostic workflow of PCa.
AI and PI-RADS scoring
PI-RADS scoring is, in its core, a classification technique. For that reason, it is believed that AI, for example with Convolutional Neural Networks which have been shown to be specifically suited for classification tasks, can be better than humans at categorizing9.
While the jury is still out to prove whether that is correct, advancements in AI radiology software show that there are different ways in which AI can support the radiologist to determine a PI-RADS score. The support can range from full automatic determination of the PI-RADS score by the software to AI-driven guidance for the radiologist in each of the PI-RADS system categories.
AI software as a PI-RADS scoring guide
Firstly, AI software can guide the radiologist through every essential input needed to make a determination of a PI-RADS score and through the guidelines v2.1, making sure the radiologist sticks to the current standard for PI-RADS classification. This type of software functions more or less as a decision tree, serving as a mnemonic tool for the radiologist.
Examples of such can be software that provides an in-software PI-RADS sketch to mark the lesion location combined with multiple categories for the radiologist to provide input while still assessing the scans. Another option is for the software to incorporate warnings when a phenomenon might have been overlooked. For example, if a radiologist marks a final score of PI-RADS 4 while the lesion has a diameter greater than 1.5cm, the program will provide a pop-up warning that this indicates a PI-RADS 5 score (note that this does mean that the software should either determine the diameter as well, or that the user has to add this information to the software).
AI software as a radiology tool for PI-RADS scoring support
Radiologists can also find software that falls in the middle of the road. Even though the final PI-RADS score determination is up to the radiologist, such AI software will provide support by mapping out and providing information needed for the scoring process. For example, since PI-RADS classification is dependent on the lesion location, an program that is able to segment the prostate and its subregions can be extremely helpful for the radiologist.
Other software available in the market outputs the automatic and AI-driven prostate and lesion measurements and volumetry. These parameters affect the PI-RADS score, however, measuring them manually can be quite complicated, hence, an automated tool to assist can be very valuable.
Additionally, AI software has the potential to provide kinetic curves based on the DCE sequence. These curves can quickly and easily give away if a suspicious area resembles a tumor, for example, if the curve of that suspicious area presents a rapid upstroke and then a reasonably rapid downstroke, this is an indicator of tumor vascularity. Yet another feature that can be extremely useful for PI-RADS determination.
Discover Quantib®Prostate, our radiology AI software for optimizing the prostate MRI reading process and provides PI-RADS scoring support.
AI software for PI-RADS lesion classification
AI algorithms can be trained to output a PI-RADS score directly10 based on different parameters. Even though these are complicated to be approved by regulation bodies and its application for clinical practice has proven to be challenging, there are currently many examples in academia that show the potential of using radiomics for the attribution of PI-RADS scores.
Research has shown that radiomics features, when added to a machine-learning system, improved the diagnostic performance of PI-RADS determination (with a sensitivity of 94.4% in PZ and 91.6% in TZ)11.
Other research12,13 used radiomics to develop software that can differentiate between significant prostate cancer and nontumor cases amongst lesions with a PI-RADS 3 classification. A very promising application, as the implications of PI-RADS 3 are not always clear.
AI software for teaching PI-RADS scoring
Last but not least, it is well known that reading prostate MRI correctly, and therefore, correctly determining a PI-RADS score requires a lot of expertise14. Besides that, it has also been noted that the PI-RADS system is also difficult and time-consuming to teach3. Therefore, there is potential to use this type of AI software to support inexperienced radiologists in their training as a way to steepen their learning curve.
Conclusion
We have seen that PI-RADS assessment is a not a straightforward task and can benefit greatly from the application of AI. Improving reader agreement as well as the accuracy of prostate cancer diagnosis, adding in treatment-decisions, and helping to identify prognostic outcomes, are examples of how AI can support the many steps of the diagnostic pathway for prostate cancer.
Introducing AI to support PI-RADS determination specifically has the potential to benefit radiologists and positively affect the diagnostic path as a whole. The process may be accelerated and has the potential to be simplified, therefore minimizing the risk of mental fatigue and burnout. Additionally, quicker access for urologists to radiology results and reports will be part of the options, hence, there is potential for patients to enjoy accelerated and optimized care.
Bibliography
- Drost, F.-J. H. et al. Prostate Magnetic Resonance Imaging, with or Without Magnetic Resonance Imaging-targeted Biopsy, and Systematic Biopsy for Detecting Prostate Cancer: A Cochrane Systematic Review and Meta-analysis. European Urology 77, 78–94 (2020).
- Ahmed, H. U. et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. The Lancet 389, (2017).
- Steiner, E. Quantib’s Lunch and Learn Webinar. (2022).
- ACR, ESUR & AdMeTech. PI-RADS ® Prostate Imaging-Reporting and Data System Version 2.1. (2019).
- Schoots, I. G. MRI in early prostate cancer detection: how to manage indeterminate or equivocal PI-RADS 3 lesions? Translational Andrology and Urology 7, 70–82 (2018).
- Mussi, T. C. et al. Interobserver Agreement and Positivity of PI-RADS Version 2 Among Radiologists with Different Levels of Experience. Academic Radiology 26, 1017–1022 (2019).
- Scialpi, M. et al. Simplified PI-RADS (S-PI-RADS) for biparametric MRI to detect and manage prostate cancer: What urologists need to know. Türk Üroloji Dergisi/Turkish Journal of Urology 47, 175–182 (2021).
- Alqahtani, S. et al. Prediction of prostate cancer Gleason score upgrading from biopsy to radical prostatectomy using pre-biopsy multiparametric MRI PIRADS scoring system. Scientific Reports 10, 7722 (2020).
- Sarvamangala, D. R. & Kulkarni, R. v. Convolutional neural networks in medical image understanding: a survey. Evolutionary Intelligence 15, 1–22 (2022).
- Sanford, T. et al. Deep‐Learning‐Based Artificial Intelligence for PI‐RADS Classification to Assist Multiparametric Prostate MRI Interpretation: A Development Study. Journal of Magnetic Resonance Imaging 52, 1499–1507 (2020).
- Wang, J. et al. Machine learning-based analysis of MR radiomics can help to improve the diagnostic performance of PI-RADS v2 in clinically relevant prostate cancer. European Radiology 27, 4082–4090 (2017).
- Hou, Y. et al. A radiomics machine learning-based redefining score robustly identifies clinically significant prostate cancer in equivocal PI-RADS score 3 lesions. Abdominal Radiology 45, 4223–4234 (2020).
- Giambelluca, D. et al. PI-RADS 3 Lesions: Role of Prostate MRI Texture Analysis in the Identification of Prostate Cancer. Current Problems in Diagnostic Radiology 50, 175–185 (2021).
- Rosenkrantz, A. B. et al. The learning curve in prostate MRI interpretation: Self-directed learning versus continual reader feedback. in American Journal of Roentgenology vol. 208 W92–W100 (American Roentgen Ray Society, 2017).