In the era of preventive healthcare, early diagnosis and non-invasive treatments are the key to success. As a result, the imaging community has experienced an exponential increase of procedures performed yearly throughout the different disciplines.
With this increase in production, workload management is becoming an important factor. The amount of exams that require the attention of radiologists is increasing while the amount of hours the radiologists have in a day remains the same. It has been proven that this can affect the wellbeing of radiologist materializing in burnout1. The decreased productivity of radiologists suffering from burnout will have a negative effect on the department’s productivity thus creating a vicious cycle. This will eventually impact the quality of the clinician’s work and the general care provided to patients2.
In this article, we will cover what productivity entails in radiology, how is it normally measured and what alternatives could there be to these traditional indicators. We will also address the myriad of innovative solutions, such as artificial intelligence (AI) radiology software, that promise clinicians to increase their productivity and how can they do that.
Productivity in radiology
In radiology, productivity can be considered as the output of a physician per unit of time. It is generally used to assess the physician’s efficiency and in some healthcare systems, it is the base for the compensation scheme3. In theory, this parameter should be relatively easy to measure, however, in reality this entails a lot of complexity, variability and subjectivity.
To understand the different models commonly used to measure productivity and their disadvantages, it is important to know that the daily workflow of a radiologist consists of image-interpretive tasks (IITs) and non-image-interpretive tasks (NITs)1. The latter include highly time-consuming activities, such as administrative tasks or consultations with referring physicians, that are not directly related to the imaging assessment but are essential in order to deliver high quality patient care.
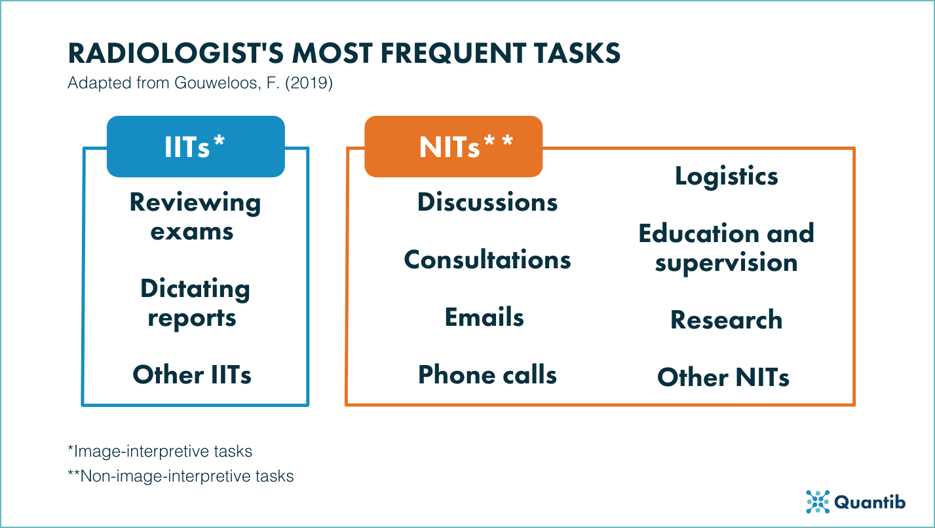
Figure 1: Summary of IITs and NITs in MR imaging4.
How is productivity commonly measured in radiology?
Traditionally, clinical productivity in the radiology field is measured with a resource-based relative value scale. This scale assigns work Relative Value Units (wRVUs) to the tasks of a professional in the medical industry1,3. These wRVUs are meant to reflect the time and effort a physician spends to do their work3.
This scale system was designed to allow for productivity comparison between medical specialties1, which is the main benefit of this system, as the practitioner’s work doesn’t necessarily align between specialties. This model standardizes productivity measurements and interorganizational comparisons3 through a set of benchmarks.
Limitations of current productivity assessment model
The main limitation of the resource-based relative value scale is that it doesn’t take into account every task radiologists perform in their workflow5. This model generally excludes NITs, like administrative tasks, as they are difficult to track and measure. However, as we stated previously, these compile a large amount of the time a radiologist spends on each case, making them equally important in the measurement of productivity.
Another limitation of this model is the delay between the emergence of a procedure and its assignment of an wRVU1.
Lastly, this model doesn’t take into account subjective factors that might have an impact on the quality and quantity of a radiologist’s work, such as exhaustion, general distractions during the day or emotional distress.
Alternatives to the traditional method to measure productivity
Some believe that an alternative would be creating a model based on the effective reading time of the radiologist instead of their general reading time. A way of measuring this would be by calculating the average effective reading time per physician’s shift, taking into account their own productivity to get a personalized benchmark per radiologist 5.
Another way of measuring productivity is calculating the physician’s report turnaround time (TAT)1, which is the time a radiologist needs to read, interpret and generate the report of an exam. We recommend to follow this method as it allows the existence of industry-wide benchmarks that can be used in cost-effectiveness analyses while it also takes into account every single task the radiologist needs to do to get the radiology report in the hands of the referring physician (from when a exam arrives to the PACS to postprocessing, dictation etc.).
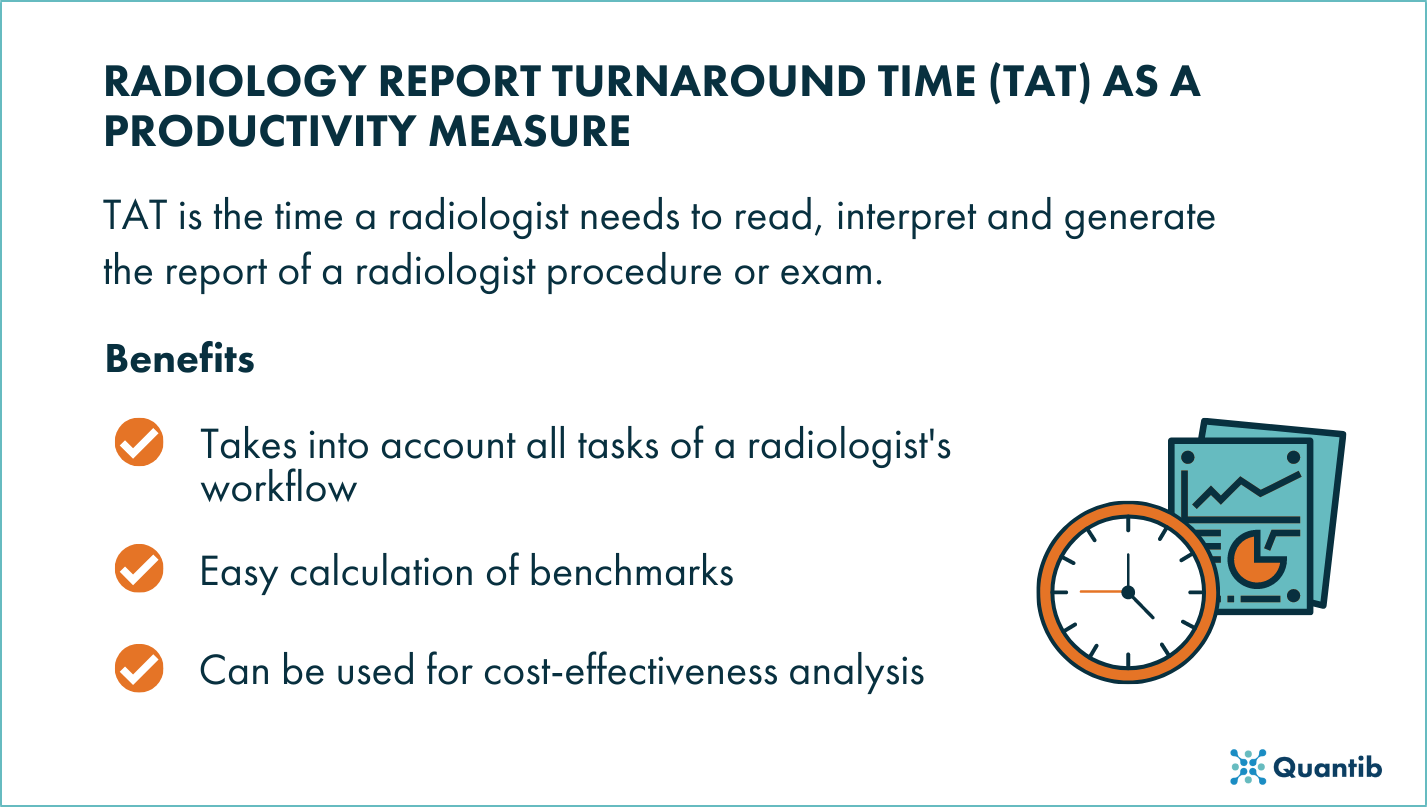
Figure 2: TAT model infographic.
Other aspects that have an impact in productivity in the radiology field
Besides the radiologist’s tasks, there are certain real factors that can affect the physician’s productivity but are not necessarily measured in any model. Therefore, these factors should be taken into account and should be stated when measuring productivity as they can have an impact on the results.
Something that will directly impact the productivity in the radiology field is the experience of the radiologist. Reading imaging exams can be a difficult task and doing so with a certain level of ease and confidence can take years of experience. Therefore, it is safe to assume that, the greater the experience of a radiologist, the lower the reading time will be (without negatively affecting the accuracy of the differential diagnosis).
Something that can have an impact on productivity has been defined by behavioral studies as the Hawthorne Effect5,6. This effect is based on the proven principle that people are more productive when they are being monitored6. This means that just the awareness of a physician’s work being observed and measured can drive the physician’s motivation to do more, faster.
Whether it might be to avoid reading difficult cases or to maximize their wRVU impact, some radiologists might be tempted to skip picking up the scan at the top of the worklist. This practice is known as cherry picking and will lead to an inevitable decrease of the productivity of the radiologist and the clinical facility5.
Lastly, pushing physicians to go faster or setting them a strict TAT they need to stick to, can have a negative impact on productivity1. The extra stress can lead to burnout, which will end up hurting productivity even harder. On the other hand, each case is different, so imposing a strict TAT might reduce the number of scans a physician reads a day or rush the assessment of difficult cases.
Can we increase productivity in radiology while maintaining the quality of care?
Innovation in healthcare is key for increasing productivity. In recent years, there has been an exponential increase of AI software available for clinical use, and that is not coincidence. AI can be applied to routine and time-consuming tasks such as volume measurement or structure segmentation which will free up time for the radiologist to use for more value-adding tasks such as consulting or training1.
AI algorithms can be applied to different steps of the clinical workflow so the implementation of AI solutions to the clinical practice is a big step towards increased efficiency and consistent quality of care.
An example: Radiology AI software for prostate MRI
We believe AI can solve the most frequent challenges radiologists face when reading prostate MRI.
AI software for prostate MRI can streamline the workflow, for example, by automatically calculating PSA density, providing an automated processing of multiple MRI sequences or providing step-wise guidance for the determination of the PI-RADS score.
Due to the automatic nature of the software, AI can help reduce the intra-observer variability as the results won’t be affected by the radiologist’s stress and mental fatigue which can increase the efficiency of the radiologist’s workflow.
Some radiology AI software for prostate MRI reading include the generation of a standardized radiology report. This has a lot of benefits because the report will be generated faster and will include everything the treating physician in the prostate cancer diagnostic workflow needs to know to make further treatment decisions. This can be a big step towards improving communication between peers and between physicians and their patients thus increasing the overall quality of care.
And the best thing about AI software is that it allows the radiologist to perform most of their tasks in a single platform, making their whole workflow more efficient as it decreases the amount of different software needed.
Discover Quantib®Prostate, our radiology AI software for optimizing the prostate MRI reading process.
![]()
Conclusion
The increase of imaging workload physicians face is a reality, and with that, so is the clinical need of increasing productivity across their workflows.
However, the most traditional method to measure productivity and do cost-benefit analysis in radiology doesn’t adjust to this new reality. The resource-based relative value scale is too strict, because it excludes important tasks from the calculation, and too inflexible, because it takes a long time for it to include emerging tasks and technologies.
As healthcare is transitioning (or, in some cases, has already transitioned) from being volume-based to being value-based, it is essential to find ways of measuring the NITs that provide value, instead of volume (non wRVUs) 1.
For that reason, we believe that measuring productivity should be done with models that take a more holistic approach, like the TAT model does.
Moreover, the implementation of innovative solutions to better manage that workload is necessary to avoid emotional distress, such as burnout, and to maintain high quality standards of patient care.
Bibliography
- Griffith, B., Kadom, N. & Straus, C. M. Radiology Education in the 21st Century: Threats and Opportunities. Journal of the American College of Radiology 16, 1482–1487 (2019).
- Chetlen, A. L. et al. Addressing Burnout in Radiologists. Academic Radiology 26, 526–533 (2019).
- Ding, A., Saini, S. & Berndt, E. R. Radiologist Productivity: What, Why, and How. Journal of the American College of Radiology 6, 824–827 (2009).
- Gouweloos, F. A. et al. Quality and efficiency within radiology and the added value of a regional PACS. (2019).
- Eggleston, P. & Bergey, E. A. The Good, the bad and the ugly: Radiology Productivity and Quality Metrics. AuntMinnie Webinars (2021).
- Kidwai, A. S. & Abujudeh, H. H. Radiologist Productivity Increases With Real-Time Monitoring: The Hawthorne Effect. Journal of the American College of Radiology 12, 1151–1154 (2015).